Abstract
Due to their vulnerability, children need special protection from health effects of climate change, which are already noticeable today. Since a large proportion of children in Germany are in non-parental care during the day, the pedagogical staff in daycare centers play a crucial role in protecting children’s health. For this reason, a quantitative online survey was conducted among pedagogical staff (n = 181) in daycare centers of one provider in Munich, where children aged nine weeks to 10 years are cared for. It was examined how the pedagogical staff assesses the risk of climate change-related health hazards on children’s health and on its own health at work today and in the next 10 years. Additionally, it was surveyed whether or which measures for (health-related) adaptation to climate change and long-term climate change mitigation in the form of education for sustainable development (ESD) are implemented in the daycare centers. The results were statistically analyzed both descriptively and with multiple linear regression analyses to test the assumed associations. The results show that despite the strong perception of climate change-related health risks, their implementation in corresponding protection and adaptation measures is insufficient in most of the daycare centers surveyed. The informedness of the pedagogical staff proved to be a decisive influencing factor in the implementation of measures. Therefore, in addition to stronger implementation of structural adaptation measures in daycare centers, target group-specific knowledge and instructions for action should also be increasingly conveyed in the training curricula and further education of pedagogical staff.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Climate change is already having a variety of direct and indirect negative impacts on human health and will continue to do so in the future. On the one hand, it can be assumed that already existing health problems that are influenced by climate conditions will increase in frequency and severity. On the other hand, climate change leads to health hazards appearing in places that were not previously affected by them. Furthermore, these shifts can cause multiple health threats to occur simultaneously, leading to cascading or mutually reinforcing impacts (Crimmins et al. 2016).
In Germany, climate change-related adverse effects on human health are already noticeable particularly through an increase in heat waves and the associated increase in thermal stress (Augustin et al. 2017; Mertes et al. 2021). Due to their limited functioning thermoregulatory system, heat dissipation in children leads to increased cardiac output, making them particularly vulnerable to respiratory and renal disease, electrolyte depletion, and fever during heat stress (Watts et al. 2019; Anderko et al. 2020).
The climate change-induced rise in temperature also influences behavioral patterns, such as leisure activities, and leads to increased time spent outdoors. This increases individual UV exposure (Eis et al. 2010; Augustin et al. 2017). Infants, children, and adolescents are particularly at risk from UV radiation, as sunburns in childhood and adolescence increase the risk of skin cancer two to three times over the course of a lifetime (Federal Office for Radiation Protection 2021).
Furthermore, extreme weather events, such as floods, heavy precipitation, droughts, and storms, can result not only in direct physical effects, but also in mental health impacts, which have often been underestimated so far (Watts et al. 2019). Climate change impacts may also lead to indirect psychological effects even without directly experiencing an extreme event, which can cause negative emotions and symptoms such as panic attacks, loss of appetite, obsessive thinking, and insomnia (Usher et al. 2019; Stanley et al. 2021).
Allergic diseases are also influenced by climate change. Higher CO2 concentrations in the atmosphere and warmer average temperatures lead to an increase in pollen production, a prolonged pollen count (Traidl-Hoffmann 2021; Wolf et al. 2021) and the spread of invasive animal and plant species (e.g., ragweed, oak processionary moth) (Heudorf 2011; Augustin et al. 2017).
Furthermore, air quality is also affected by anthropogenic climate change and has a negative impact on human health. Particularly relevant for human health are air pollutants such as ozone (O3), particulate matter (PM), and nitrogen dioxide (NO2) (Wolf et al. 2021). An intensification of the negative influence of air pollutants on health at higher air temperatures has already been scientifically proven (Katsouyanni et al. 2001; Rai et al. 2023).
Changing climatic factors also affect pathogens and their vectors and thus influence the occurrence of infectious diseases. Vector-based infectious diseases in Germany are primarily transmitted to humans by mosquitoes and ticks. Besides the lower natural decimation of native mosquito or tick populations due to milder winters, vectors can also spread further north as well as in higher regions (Augustin et al. 2017). Moreover, “new” infectious diseases are becoming established in Germany, as the rise in temperature creates new habitats for vectors (e.g., Asian tiger mosquito Aedes albopictus) (Semenza and Suk 2018; European Centre for Disease Prevention and Control 2020; Wolf et al. 2021).
In addition to pregnant women, the elderly, and people who work outdoors, (young) children are particularly vulnerable to the health effects of climate change (Augustin et al. 2017; Watts et al. 2019). In dealing with these risks, children are dependent on the health-related skills of adults. For example, up to a certain age, discomfort as a result of feeling hot or thirsty can only be expressed to a limited extent (Garcia and Sheehan 2016).
In Germany, around 3.9 million children are cared for in daycare centers (Bavarian State Ministry for Family, Labor and Social Affairs 2020). The pedagogical staff in daycare centers has a great influence on the health of children due to diverse care, upbringing and educational tasks (Mücke et al. 2013). Regarding the health effects of climate change, adequate assessment and knowledge of how to deal with these risks on the part of the pedagogical staff in daycare centers is therefore crucial to protect children’s health in the best possible way through (health-related) climate change adaptation. Since the pedagogical staff is exposed to the same environmental conditions during their work, the health protection of the staff at the workplace is equally important. Furthermore, in their function as educational settings, daycare centers have great potential in the field of education for sustainable development (ESD) to tackle climate change in the long term. Through ESD in the context of early childhood education, values and skills such as self-efficacy and participation are to be conveyed through the age appropriate examination of future-relevant topics, in order to enable people to think and act responsibly and sustainably (Federal Ministry of Education and Research 2022). Thus, pedagogical staff is an important multiplier both for the transfer of knowledge and values and for the promotion of relevant behaviors and adaptation measures (Mücke et al. 2013).
However, an extensive literature research on this topic and target group in various scientific databases such as PubMed and Google Scholar revealed that there are no scientific publications on the risk perception of the pedagogical staff and the handling of climate change-related health risks in daycare centers in Germany so far. A gray literature could be found, which was published in the context of a German research project. In this, the management level of 105 German facilities in the health and care sector, including 51 daycare centers, was surveyed on the handling and risk perception of environmental health risks, today and in the next 10 years. Heat waves were seen as the greatest health risk by about three-quarters of the facilities surveyed, both today and in the future. These were followed by particulate matter (today: 43%, in the future: 35%), influenza and other epidemics (today: 42%, in the future: 33%), heavy rain and flooding (today: 46%, in the future: 41%), and storms, thunderstorms, hail (today: 39%, in the future: 35%) as perceived health risks. Moreover, the survey asked which structural measures against heat are already in place in the facilities. In the surveyed daycare centers, the main heat protection measures were sun protection/darkening (80%), a garden or green courtyard (75%), insulation of roof or facades (50%), water areas and fountains (35%), and fans (30%). Less than 20% of the daycare centers had thermal glazing/foil or green roofs and facades, and none had air conditioning. Especially daycare centers wanted more target group-specific information and advice on dealing with heat, as they felt only moderately informed on the topic (Ullrich et al. 2020). Besides these project results, some internal guidelines of different providers of daycare centers were found, especially on dealing with heat, floods, vectors such as mosquitoes and ticks, as well as climate protection (e.g., Thielebein et al. 2019; Johanniter-Unfall-Hilfe e.V. 2020; Deutscher Paritätischer Wohlfahrtsverband 2022).
The limited international data available on dealing with climate change health risks in daycare centers consistently indicate that pedagogical staff do not adequately assess environmental and climate change-related risks to children’s health mostly due to lack of knowledge and awareness (Amoah et al. 2016; Folkerts et al. 2020; Koester et al. 2021). For example, a Dutch study examined the abilities of caregivers in daycare centers to assess children's heat sensations and to recognize heat-related symptoms (Folkerts et al. 2020). It was found that especially persons with less than 5 years of professional experience had little knowledge about children’s thermoregulation compared to persons with many years of professional experience and had difficulties in naming heat-related symptoms specifically. About 30% of the 58 caregivers interviewed from six different facilities believed that thermoregulation of children and adults did not differ. In addition, 23.5% could not spontaneously name any symptom of heat-related illness. In this context, the lack of such content in the training curricula was repeatedly pointed out by the participants during the interviews, which, according to the researchers, could be an explanation for the knowledge deficits among persons with little professional experience (Folkerts et al. 2020). A pilot project in the USA that provided targeted training for pedagogical staff on environmental health hazards demonstrated that increased knowledge on this topic was associated with increased and improved protective measures for children’s health (Amoah et al. 2016). The authors of these studies therefore emphasize the need to increase knowledge and awareness regarding environmental health hazards on the part of pedagogical staff in order to better protect the children in their care (Amoah et al. 2016; Folkerts et al. 2020; Koester et al. 2021).
In order to contribute to closing this research gap with regard to the aforementioned aspects in Germany, the present study was conducted among pedagogical staff in daycare centers of one provider in Munich. The focus was on answering the following research questions:
-
1.
How do pedagogical staff in daycare centers perceive the risk of climate change-related health hazards for children’s health and for their own health at the workplace today and in the next ten years?
-
2.
Are measures for (health-related) climate change adaptation and mitigation already implemented in the daycare centers?
-
3.
Is there an association between risk perception and the implementation of measures or other influencing factors?
Methods
The present study is a regional online survey of pedagogical staff in daycare centers of one provider in Munich. The online questionnaire with 21 questions was sent by the daycare provider to about 6000 persons in more than 400 facilities between November 25, 2021, and January 31, 2022. The daycare centers surveyed care for children between the ages of 9 weeks and 10 years.
Questionnaire design
The first part of the questionnaire collected information about the workplace of the participants (age of the children in care, personal work area, number of children cared for, postal code of the daycare center). Personal attitudes toward climate change were assessed by statements about the effects (global or national) and the cause (natural or man-made) of climate change, as well as with the help of the items “climate change is a major social challenge.” and “climate change and its consequences worry me.” These were to be rated using a four-point Likert scale (1 = “strongly disagree”; 2 = “rather disagree”; 3 = “rather agree”; 4 = “strongly agree”). In order to determine the extent to which the pedagogical staff is already informed about the topic of climate change and health, it was asked whether or which sources of information were used actively and for professional reasons to obtain information (given choice of answers: “no sources of information,” “newspaper,” “magazines,” “radio,” “television,” “books,” “internet,” “social environment,” “further training by the employer”). Multiple answers and the open input of other sources of information through the “other” option were possible. To assess the perceived affectedness of the daycare center by climate change, the pedagogical staff were asked to rate the following items using a four-point Likert scale (1 = “not at all affected”; 2 = “rather not affected”; 3 = “rather affected”; 4 = “very affected”; “don’t know”): “heat,” “heavy rain and the consequences (e.g., flooding),” “severe weather and the consequences (e.g., falling trees from storms, hail damage),” “pollen count,” “air pollutants (e.g., ozone, nitrogen oxides, particulate matter),” “mosquitoes,” “ticks.” The risk perception of climate change-related health hazards today and in the next ten years was surveyed regarding children’s health and the health of pedagogical staff at the workplace. By means of a four-point Likert scale (1 = “strongly disagree”; 2 = “rather disagree”; 3 = “rather agree”; 4 = “strongly agree”), the risk perception of the following health hazards of climate change was assessed by the pedagogical staff: heat, UV radiation, pollen count, air pollutants, mosquitoes, ticks, mental consequences due to extreme weather events (heat waves, heavy rain/flooding, storms, hail), and physical consequences due to extreme weather events (heat waves, heavy rain/flooding, storms, hail).
In order to gain an impression of the conditions in the daycare centers, it was firstly asked whether the daycare center has an outdoor area on its own property. The second question asked about the proportion of outdoor area that is unsealed (e.g., green and sand areas). Whether or which structural measures and behavioral measures are implemented in the facility to protect against the health effects of climate change was surveyed in each case using a list of different measures (see Figs. 4 and 5). Regarding pedagogical measures for long-term climate change mitigation through education for sustainable development (ESD), it was surveyed whether certain topic areas of climate protection and sustainability are implemented in the pedagogical work (see Fig. 6). In each case, there was the option for multiple answers as well as the use of an “other” option to add further measures implemented. In the last part, the participants were asked about socio-demographic details (age group, gender, type of vocational training/study).
Statistical analysis
Since the third research question aims to determine associations between the risk perception of pedagogical staff and the implementation of adaptation and mitigation measures, as well as to identify other influencing factors, the following concretizing hypotheses were derived, which are presented in a graphical hypothesis model in Fig. 1:
-
Main hypothesis: There is an association between pedagogical staff’s risk perception of climate change-related health hazards and the implementation of adaptation and mitigation measures in daycare centers.
-
Sub-hypothesis 1: There is an association between the characteristics of the daycare center and the risk perception of the pedagogical staff.
-
Sub-hypothesis 2: There is an association between the personal characteristics of the pedagogical staff and their risk perception.
-
Sub-hypothesis 3: There is an association between the characteristics of the daycare center and the implementation of adaptation and mitigation measures.
-
Sub-hypothesis 4: There is an association between the personal characteristics of the pedagogical staff and the implementation of adaptation and mitigation measures.

Hypothesis model based on third research question
For testing the main hypothesis, a correlation of 0.25 was considered relevant. This required a sample size of n = 164 with a significance level of α = 0.05 and a 2nd kind error of β = 0.1 (Ackermann 2006). The inclusion criteria were having a caring or pedagogical position and answering ≥ 50% of the questionnaire. Exclusion from the sample occurred in the absence of having a caring or pedagogical role and answering < 50% of the questions in the questionnaire.
The statistical analysis of the data was performed with R Statistical Software, version 4.1.2. (R Core Team 2021). For descriptive analysis, the mean (M) and standard deviation (SD) were determined. The four-point Likert scales were evaluated using the scale mean values. For questions with a “don’t know” option, the evaluation of this option took place separately. In addition, correlative associations were calculated using Pearson’s correlation coefficient. The significance level was α = 0.05. Despite the ordinal scaled response options of the Likert scales, the use of parametric tests is permissible (Norman 2010; Sullivan and Artino 2013). To test the assumed associations in the hypotheses, five multiple linear regression models were performed. The prerequisites for regression analyses were checked by testing for homoscedasticity, normal distribution of the residuals, linearity, outliers, and the absence of multicollinearity (Bortz and Schuster 2011). In addition, single factor analyses of variance (ANOVA) were performed to test model fit and significance for the respective models (see Table 2). Associations with a significance level of p < 0.05 were accepted as statistically significant. To meet the requirement of a metric outcome measure in the regression models, sum scores were created from actively used sources of information and the structural, behavioral, and educational measures implemented, corresponding to the number of given response options (e.g., 12 response options for structural measures taken in the questionnaire: possible score 0–12), without weighting them according to quality. In addition, to calculate the regression models, the risk perception on children’s health and health of the pedagogical staff, the affirmative attitude toward climate change, and the facility’s affectedness were each summarized in scores. To better compare the variables as coefficients in the regression models, a z-standardization of all formed scores was performed in advance.
Results
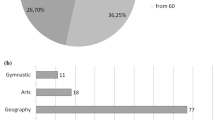
At the end of the survey period, 256 responses had been received. Considering the inclusion and exclusion criteria, 75 responses had to be excluded, resulting in a representative sample size of n = 181 persons from 57 different postal code zones. Postal code zones located on the Munich city border were grouped into suburban location (40.9%). The remaining postal codes formed the inner-city location group (53.0%). 6.1% of the participants did not specify the postal code of their facility. Since, for data protection reasons, only the postal code of the daycare center could be collected to determine the location, it is therefore not possible to draw any conclusions about individual facilities. The sample was composed of 85.6% female and 8.3% male participants. 6.1% of the respondents did not provide any information on their gender. 81.2% of the surveyed pedagogical staff were working in facilities caring for 0- to 6-year-old children. 18.8% of respondents cared for children aged 7 to 10.
Descriptive analysis results
Attitudes toward climate change
The analysis of the attitudes of the pedagogical staff toward climate change showed that 94.5% of the respondents agreed with the statement that climate change is already happening globally (“rather agree”: 18.8%; “strongly agree”: 75.7%). The level of agreement that climate change is already taking place in Germany was 91.2% (“rather agree”: 28.2%; “strongly agree”: 63.0%). In addition, 50.3% fully agreed that climate change is man-made, while 41.4% rather agreed with this statement. 87.3% of respondents felt concerned by climate change and its consequences (“rather agree”: 31.5%; “strongly agree”: 55.8%), while a total of 12.7% did not or rather did not feel worried.
Sources of information about climate change and health
Furthermore, participants were asked about their sources of information on climate change and health that they used actively and for professional reasons. The most frequently mentioned sources of information were television (49.7%), the social environment (43.1%), newspapers (39.8%), and the Internet (38.7%). 22.7% of the pedagogical staff stated that they did not use any of the mentioned sources to inform themselves about this topic.
Perceived affectedness of the daycare centers by climate change
Additionally, the pedagogical staff was asked about how affected their facility is by various effects of climate change. Perceived affectedness comparing inner-city and suburban locations are shown in Fig. 2. The impacts of air pollutants, pollen count, and heat were rated highest by both inner-city and suburban daycare centers. There was uncertainty on the part of the pedagogical staff regarding the assessment of being affected by pollen count. The option “don’t know” was mentioned most frequently in this context with 14.1%. Further uncertainties also existed regarding the extent to which the daycare centers were affected by ticks (12.3%) and mosquitoes (10.6%).

Perceived affectedness of the facility (mean value; suburban location: n = 74; inner-city location: n = 96). Question: “How do you think the district where your facility is located is already affected by…?” (Response options: 1 = “not at all affected”; 2 = “rather not affected”; 3 = “rather affected”; 4 = “very affected”)
Risk perception
The aim of the first research question was to gain insights into pedagogical staff’s risk perceptions of climate change-related health hazards to children’s health and their own health at the workplace today and in the next ten years. Overall, the results show that respondents rated most of the given climate change-related health risks slightly higher for children’s health than for their own health (see Fig. 3). Participants saw the greatest risks to children’s health and their own health today from UV radiation (children’s health: M = 3.39; SD = 0.80; pedagogical staff health: M = 2.93; SD = 0.96), air pollutants (children’s health: M = 3.29; SD = 0.85; pedagogical staff health: M = 3.10; SD = 0.91), and heat (children’s health: M = 3.04; SD = 0.97; pedagogical staff health: M = 2.87; SD = 1.05). Risks from physical and mental consequences due to extreme weather events were rated lowest. It was also found that the “don’t know” option was used more frequently by pedagogical staff in relation to risk perceptions for children’s health than for their own health. Especially regarding risks to children’s health from mental and physical consequences due to extreme weather events (mental consequences: 9.4%; physical consequences: 9.4%), the “don’t know” option was used about two and three times more frequently than for their own health (mental consequences: 5.0%; physical consequences: 3.3%). Overall, most “don’t know” responses were given regarding risk from ticks (children’s health: 12.2%; pedagogical staff health: 8.8%), pollen count (children’s health: 11.6%; pedagogical staff health: 7.7%), and mosquitoes (children’s health: 11.0%; pedagogical staff health: 6.6%).

Comparison of perceptions of climate change-related health risks today (mean; n = 181). Questions: “To what extent do you see a risk to the health of the children in your facility due to…?” or “To what extent do you see a risk to your own health at work due to…?” (Response options: 1 = “strongly disagree”; 2 = “rather disagree”; 3 = “rather agree”; 4 = “strongly agree”)
Regarding the perception of the questioned health risks in the next 10 years, there was an increase in all items. Pedagogical staff perceived future health risks to be higher for children’s health than for their own health. However, it was noticeable that the difference between the risk perception was smaller compared to the risk perception today. Future perceived health risks for both children’s health and own health were highest for air pollutants (children’s health: M = 3.57; SD = 0.71; pedagogical staff health: M = 3.42; SD = 0.85), UV radiation (children’s health: M = 3.57; SD = 0.76; pedagogical staff health: M = 3.26; SD = 0.95), and heat (children’s health: M = 3.48; SD = 0.81; pedagogical staff health: M = 3.25; SD = 0.95). An overall increase was also found in the use of the “don’t know” option regarding future health risks. The percentage differences between the “don’t know” responses for children’s health and for those of the pedagogical staff were smaller than for the perception of today’s health risks. The option was most frequently used for risks from pollen counts (children’s health: 16.0%; pedagogical staff health: 12.4%), mosquitoes (children’s health: 16.0%; pedagogical staff health: 14.0%), and ticks (children’s health: 14.9%; pedagogical staff health: 15.7%).
Implementation of adaptation and mitigation measures
Answering the second research question was intended to clarify whether and which measures for (health-related) climate change adaptation and mitigation are already being implemented in the facilities. A distinction was made between structural and behavioral measures (adaptation) as well as between pedagogical measures in the sense of integrating topics in the field of education for sustainable development (ESD) into the pedagogical work (long-term mitigation). Regarding the implementation of adaptation measures for health protection, about 40% of the daycare centers stated that they had not yet implemented any structural measures (see Fig. 4) and 19.3% had not implemented any behavioral measures (see Fig. 5). The main focus of the implemented structural and behavioral protection measures was on heat and UV protection. Shading in the outdoor area (e.g., by sun sails and sunshades) was the most frequently named structural protective measure with 54.5%, followed by darkening of indoor areas (e.g., by roller blinds, curtains) with 52.8%. Thus, the most frequently mentioned measures were only implemented in every second facility. Active cooling of the indoor area by fans (7.4%) or air conditioning (2.8%) was carried out in only a few daycare centers. Thermometers for indoor and outdoor temperature measurement were present in 14.8% and 8.5% of the facilities. The most common behavioral measures were changes in the time spent outdoors because of heat (69.9%), taking more frequent or fixed drinking breaks (56.3%), and providing sunscreen products (50.6%) and sun protective clothing (44.9%). Despite the overall high level of concern about air pollutants, only 15.9% of facilities had adjusted the time spent outdoors to account for air pollutant concentrations. Further training opportunities on climate change and health protection by the employer were available in 14.8% of facilities, but these were only used by 8.8% of respondents.

Structural measures taken to protect against health effects of climate change (percentage distribution; n = 176). Question: “Are structural measures to protect against health effects of climate change being implemented or planned in your facility in the near future? If yes, which ones?” (Multiple answers possible from given answers)

Behavioral measures taken to protect against health effects of climate change (percentage distribution; n = 176). Question: “Are climate change-related behavioral measures to protect health at your facility being implemented or planned in the near future? If yes, which ones?” (Multiple responses possible from given answers)
In order to find out which measures for long-term climate change mitigation are implemented in the daycare centers, the pedagogical staff was also asked to what extent topics in the field of ESD are part of the pedagogical work with the children. 9.2% of the participants stated that they did not deal with any of the given topics (see Fig. 6). Health topics were mentioned most frequently with 80.5%, followed by waste separation and recycling (64.9%), nature and environmental education (63.8%), and the conscious use of energy and resources (59.8%). Especially in comparison to the other given topics, it was noticeable that the topic of climate change with 17.2% was by far the smallest part of the pedagogical work in the field of ESD.

Integration of topics in the field of education for sustainable development (ESD) in the pedagogical work (percentage distribution; n = 174). Question: “Are the following aspects of climate protection or sustainability part of the pedagogical work in your facility? If yes, which ones?” (Multiple answers possible from given answers)
Results of correlation and regression analyses
In the context of the third research question, a correlation matrix and five regression models were used to test the assumed associations. For the calculations, the item “informedness” of the pedagogical staff was operationalized by the score of actively used sources of information on climate change and health.
Correlation matrix
The correlation matrix (see Table 1) shows that a positive correlation was found between pedagogical staff’s informedness and their attitudes toward climate change, the facility’s perceived affectedness by climate change impacts, risk perceptions for children’s health today, and the implementation of adaptation and mitigation measures, but not with risk perceptions for the staff’s own health at work. In addition, the facility’s affectedness to climate change impacts correlated with risk perception and the implementation of behavioral measures. Affirmative attitudes toward climate change also correlated positively with the implementation of structural and behavioral measures. No significant correlation was found between risk perception and implementation of adaptation and mitigation measures.
Regression models
Table 2 shows the summaries (ANOVA outputs) of the five regression models with the dependent and independent variables, as well as R2 and adjusted R2, the degrees of freedom (Res. Df and Df), and the F and p values. To calculate the outcome variable “risk perception,” risk perception for children’s health today and in the next 10 years and for the health of pedagogical staff at the workplace today and in the next 10 years were combined into a total score for the calculation of models 1 and 2. To calculate models 3, 4, and 5, a total score for the adaptation and mitigation measures taken was formed from the structural, behavioral, and pedagogical measures.
The assumption of the first sub-hypothesis, that there is an association between the characteristics of the daycare centers and the risk perception of the pedagogical staff, could be confirmed. A statistically significant influence was exerted by the daycare center’s affectedness by extreme weather events and by vectors (mosquitoes, ticks). In the context of the of the second sub-hypothesis, it was possible to prove that there is a positive association between the personal characteristics of the pedagogical staff and their risk perception, through the influence of affirmative attitudes toward climate change. No association—and thus no confirmation of the third sub-hypothesis—was found between the characteristics of daycare centers and the implementation of structural, behavioral, or pedagogical measures. The analysis of the association between the personal characteristics of the pedagogical staff and the implementation of climate change adaptation and mitigation measures (sub-hypothesis 4) showed a positive influence of the informedness of the pedagogical staff (score of used information sources) on the implementation of measures in the daycare centers. Since risk perception was itself influenced by various factors, the influential variables that had a significant effect on risk perception in models 1 and 2 (see Table 2) were included in regression model 5 to test the association between risk perception and the implementation of adaptation and mitigation measures (main hypothesis). Here, although it was found that the perceived affectedness of the daycare centers by vectors had a significant positive influence on the measures taken, no statistically significant association of risk perception on the implementation of measures could be demonstrated. This confirms the results of the correlation matrix (see Table 1).
Discussion
Relevance and novelty of the results
To the best of our knowledge, the results of the present study provide the first quantitative data on the risk perception of climate change-related health hazards as well as on the implementation of corresponding adaptation and mitigation measures in daycare centers for children in the German-speaking region, in which the pedagogical staff was directly surveyed.
With regard to answering the first research question, it was found that climate change-related health risks—especially from UV radiation, air pollutants, and heat—are rated higher by pedagogical staff for the health of children than for their own health at work, both today and in the next 10 years. In this context, it is positive to note that the increased risk to children seems to be known to the pedagogical staff. Nevertheless, strengthening staff’s self-protection at the workplace as an occupational health aspect should also be given more emphasis in the future, especially against the background that people tend to underestimate own risk compared to others (Berger et al. 2019), e.g., because they are not aware of their own risk factors (Betsch et al. 2023). Part of the respondents is skeptical about climate change and does not perceive its consequences as a threat. Scientific research on this shows that individuals nevertheless acknowledge a certain level of risk when confronted with objective information (Schwarzer 2016). In terms of fulfilling the duty of care of pedagogical staff, targeted and scientifically sound communication of climate change health risks is essential to ensure the protection of children in care from climate change-related health hazards, regardless of the caregivers’ personal attitudes toward climate change.
Regarding the implementation of appropriate structural and behavioral adaptation measures to protect health, it was found that these are mainly implemented in the form of heat and UV protection measures in the facilities. Overall, despite the strong perception of affectedness and health risks, their transfer into corresponding structural and behavioral protective measures has been insufficient in most of the surveyed daycare centers so far. Particularly regarding the Occupational Health and Safety Act, the facility provider has a responsibility to protect the health of its employees. Hence, the question arises to what extent health protection can be ensured under the current conditions for both the employees and the children if insufficient adaptation to the changing climate conditions takes place. Education for sustainable development (ESD) as part of the pedagogical work for long-term climate change mitigation is taught in the facilities through various sustainability topics. However, climate change itself has so far played a minor role as a topic. Thus, although ESD issues seem to be generally familiar, they have not yet been directly related to climate change. The study findings of Berger et al. 2019 reinforce the assumption that topics relevant to climate change are not always associated with it. Particularly due to the large gap in teaching the topics of health and climate change, there is a need for increased awareness of the connections between these two issues.
Looking at the third research question, it was found that there is no significant correlation between risk perception and the implementation of adaptation and mitigation measures. This nonsignificant correlation is consistent with other study findings on the relationship between risk perception and changes in health behaviors (Milne et al. 2000). In contrast, the correlation and regression analyses show an association between the facility’s affectedness by climate change impacts and the implementation of behavioral measures. Changes in health behavior in the form of protective measures thus appear to occur in response to already perceived climate change impacts. It was also found that, in particular, the informedness of pedagogical staff is a key factor in the implementation of adaptation and mitigation measures. However, nearly a quarter of respondents said they did not obtain any information at all on this topic. Those who actively sought information most frequently used television, the social environment, newspapers, and the Internet as sources of information. These channels raise the question to what extent the knowledge acquired is based on scientifically sound information. It is also notable that while informedness correlates with risk perceptions of climate change-related health hazards to children’s health, it does not correlate with perceptions of risks to pedagogical staff’s health. In this context, a study of Betsch et al. 2023 showed that people who privately or professionally care for vulnerable persons are less informed about heat risks, even though this group is more likely to receive information about heat. This is also corroborated by survey results of Ullrich et al. (2020), which demonstrate that pedagogical staff feel only moderately informed. In line with other studies (Amoah et al. 2016; Folkerts et al. 2020; Koester et al. 2021), it is therefore important to improve the level of information of pedagogical staff through evidence-based knowledge transfer as well as practical experience in order to increase the implementation of measures. For this purpose, the inclusion of the topic of climate change and health in training curricula and further training formats for pedagogical staff would be well suited. That target group-specific information is explicitly desired by the pedagogical staff was also shown by the survey of Ullrich et al. (2020). Teaching health-related skills to pedagogical staff thus opens up further important opportunities in the context of long-term climate change mitigation: using the significant multiplier function of this professional group by transferring knowledge and adapted (health-related) behaviors directly to children and thus also indirectly to their families. The positive effect of intergenerational learning from children to parents has already been scientifically proven. Children can use the acquired knowledge and learned behaviors in the daycare center to motivate their parents to pay more attention to the issue of climate change and its consequences, as well as to the options for action (Lawson et al. 2018, 2019).
Study limitations
One limitation of the present study is that only one provider of daycare centers in one city was investigated. For further research, a nationwide survey of different providers would be useful, as the measures implemented may vary. In addition, the assessment of risk perception in this study does not cover all dimensions of risk perception or its influencing factors. Therefore, potentially crucial factors related to risk perception may not have been considered. Furthermore, the assessment of the informedness of the pedagogical staff represents a limiting factor of this study, as it was operationalized on the basis of the number of information sources used, without weighting them in terms of quality. Since informedness has been shown to be a crucial influencing factor for risk perception and implementation of measures, a targeted and differentiated assessment of the existing knowledge of the pedagogical staff regarding the topic of climate change and health could provide an approach for further research. It should also be noted that reverse causality may exist. For example, it is possible that pedagogical staff is more aware of climate change issues and more informed because it is exposed to adaptation measures or climate change hazards in the work context. Another limitation is that the survey asked whether adaptation measures had already been implemented or were planned for the near future, but this could not be differentiated in the response options. It cannot be ruled out that measures considered implemented in the evaluation are still being planned in the facilities.
Conclusion
Due to their vulnerability, children need special protection against the health risks of climate change. Since a large number of children in Germany are in non-parental care during the day, the pedagogical staff in daycare centers play a decisive role in protecting the health of children. However, this professional group is not only an important multiplier regarding the promotion of health adaptation measures. As part of the educational work in the daycare centers, imparting knowledge and values in the area of education for sustainable development (ESD) is an important component for long-term climate change mitigation. Also, for their own health protection at the workplace, distinctive health-related competences of the pedagogical staff are useful.
In order to contribute to closing the identified research gap regarding the risk perception of climate change-related health hazards by the pedagogical staff and the implementation of corresponding measures for (health-related) climate change adaptation and climate protection in the facilities, the present study was conducted exemplarily on the basis of daycare centers of one provider in Munich. With regard to the question of how the pedagogical staff perceives the risks of climate change-related health hazards to children’s health and their own health at work, it was found that the risks of UV radiation, air pollutants, and heat are estimated to be the greatest today and in the next 10 years. An overall increase in risk perception of climate change-related health hazards for the next 10 years was also noted. In addition, respondents perceived health risks to be higher for children than for themselves today and in the future. Structural and behavioral measures taken in the daycare centers were mainly in the form of heat and UV protection measures. Despite the pronounced perception of risk and the perceived affectedness of the facility by climate change impacts, deficits in the implementation of appropriate protective measures for (health-related) climate change adaptation are evident in a majority of the daycare facilities. Also, with regard to long-term climate change mitigation through ESD as part of the pedagogical work, various topics of sustainability are conveyed, but climate change itself as a topic has so far played a subordinate role. Here, the large discrepancy in the communication of the topics of health and climate change was particularly noticeable. When examining the association between risk perception and the implementation of adaptation and mitigation measures, as well as the identification of further influencing factors, it became clear that there is no direct association between risk perception and the implementation of protective measures. However, informedness (number of actively used information sources) as a personal characteristic of the pedagogical staff played a crucial role and is positively correlated with the attitude toward climate change, the assessment of the facility’s affectedness by the impacts of climate change, the risk perception for children’s health today as well as the implementation of measures.
The results of the present study provide a first overview of the risk perception of climate change-related health hazards in daycare centers, the adaptation and mitigation measures taken, and their associations. Since the risk perception alone does not lead to action, further research could start here to find out what obstacles exist to close this gap. The study also revealed needs and inadequacies in both situational and behavioral prevention that urgently need to be addressed. As a consequence for practical implementation, it should be considered not only to take reactive measures in daycare centers when the impact of climate change is already noticeable, but to act preventively, based on the individual affectedness and risk of the facility. In this context, the results highlight the relevance of informed pedagogical staff in the implementation of protective measures. This is where the integration of the topic into training curricula and further training formats can come in, where the focus is not only on the promotion of need-based knowledge and target group-specific sensitization, but also on the communication of concrete instructions for the implementation of protective measures. Well-trained and health-competent pedagogical staff is the prerequisite for fully using the multiplier function of this professional group and thus adequately protecting the health of the children in care and the staff themselves.
Data availability
The data supporting the results of this study are not publicly available for reasons of data protection and can be requested from the corresponding author upon justified request. The data are located in a controlled-access data repository at Ludwig-Maximilians-University Munich.
References
Ackermann H (2006) BiAS für Windows. https://www.bias-online.de/Manual11.pdf. Accessed 05 Dec 2022
Amoah AO, Witherspoon NO, Pérodin J, Paulson JA (2016) Findings from a pilot environmental health intervention at early childhood centers in the District of Columbia. J Public Heal (united Kingdom) 38:e209–e217. https://doi.org/10.1093/pubmed/fdv135
Anderko L, Chalupka S, Du M, Hauptman M (2020) Climate changes reproductive and children’s health: a review of risks, exposures, and impacts. Pediatr Res 87:414–419. https://doi.org/10.1038/s41390-019-0654-7
Augustin J, Sauerborn R, Burkart K, Endlicher W, Jochner S et al (2017) Health. In: Brasseur GP, Jacob D, Schuck-Zöller S (eds) Climate change in Germany. Springer, Berlin, pp 137–149
Bavarian State Ministry for Family, Labor and Social Affairs (2020) Care rates. https://www.stmas.bayern.de/service-kinder/statistik/index.php#sec1. Accessed 21 Dec 2022
Berger N, Lindemann AK, Böl GF (2019) Public perception of climate change and implications for risk communication. Bundesgesundheitsblatt - Gesundheitsforsch - Gesundheitsschutz 612–619. https://doi.org/10.1007/s00103-019-02930-0
Betsch C, Hellmann L, Sprengholz P, Shamsrizi P, Geiger M et al (2023) Planetary health action survey PACE - summary and recommendations wave 15. https://projekte.unierfurt.de/pace/_files/PACE_W15.pdf. Accessed 21 Dec 2022
Bortz J, Schuster C (2011) Statistics for human and social scientists: limited, special. Springer-Verlag
Cohen J (1988) Statistical power analysis for the behavioral sciences. https://www.utstat.toronto.edu/~brunner/oldclass/378f16/readings/CohenPower.pdf. Accessed 12 Dec 2022
Crimmins A, Balbus J, Gamble J L, Beard C B, Bell J E, Dodgen D, Eisen R J, Fann N, Hawkins M, Herring S C, Jantarasami L, Mills D M, Saha S, Sarofim M C, Trtanj J, Ziska L (2016) Executive summary. The impacts of climate change on human health in the United States: a scientific assessment. U.S. Global Change Research Program, Washington, DC pp 24. https://doi.org/10.7930/J00P0WXSOn
Deutscher Paritätischer Wohlfahrtsverband (2022) Climate protection & climate adaptation in childcare centers. https://www.der-paritaetische.de/fileadmin/user_upload/221214_Broschuere_Klimaschutz-Anpassung_in_Kitas_Web.pdf. Accessed 18 Dec 2022
Eis D, Helm D, Laußmann D, Stark K (2010) Climate change and health - a status report. https://edoc.rki.de/bitstream/handle/176904/877/29ETCuO6ZOtk.pdf?sequence=1. Accessed 19 Dec 2022
European Centre for Disease Prevention and Control (2020) Aedes albopictus - current known distribution: May 2020. https://www.ecdc.europa.eu/en/publications-data/aedes-albopictus-current-known-distribution-may-2020. Accessed 21 Dec 2022
Federal Ministry of Education and Research (2022) Early childhood education. https://www.bne-portal.de/bne/de/einstieg/bildungsbereiche/fruehkindliche-bildung/fruehkindliche-bildung. Accessed 21 Dec 2022
Federal Office for Radiation Protection (2021) Why protection from UV radiation? https://www.bfs.de/DE/themen/opt/uv/schutz/einfuehrung/einfuehrung_node.html. Accessed 21 Dec 2022
Folkerts MA, Gerrett N, Kingma BRM, Zuurbier M, Daanen HAM (2020) Care provider assessment of thermal state of children in day-care centers. Build Environ 179:106915. https://doi.org/10.1016/j.buildenv.2020.106915
Garcia DM, Sheehan MC (2016) Extreme weather-driven disasters and children’s health. Int J Heal Serv 46:79–105. https://doi.org/10.1177/0020731415625254
Heudorf U (2011) Oak processionary moth - a topic also for pediatric practice. Pädiatrische Allergol 14:31–32. https://www.gpau.de/fileadmin/user_upload/GPA/dateien_indiziert/Sonstiges/Paed._Allerg._1-11_Umwelt.pdf. Accessed 21 Dec 2022
Johanniter-Unfall-Hilfe e.V (2020) Recommendations for daycare centers on dealing with heat waves. https://www.uni-potsdam.de/fileadmin/projects/extrass/Kita_Hitze.pdf. Accessed 28 Dec 2022
Katsouyanni K, Touloumi G, Samoli E, Gryparis A, Le Tertre A et al (2001) Confounding and effect modification in the short-term effects of ambient particles on total mortality: results from 29 European cities within the APHEA2 project. Epidemiology 12:521–531. https://doi.org/10.1097/00001648-200109000-00011
Koester BD, Sloane S, Fujimoto EM, Fiese BH, Su LYF (2021) What do childcare providers know about environmental influences on children’s health? Implications for environmental health literacy efforts. Int J Environ Res Public Health 18. https://doi.org/10.3390/ijerph18105489
Lawson DF, Stevenson KT, Peterson MN, Carrier SJ, Strnad R et al (2018) Intergenerational learning: are children key in spurring climate action? Glob Environ Chang 53:204–208. https://doi.org/10.1016/j.gloenvcha.2018.10.002
Lawson DF, Stevenson KT, Peterson MN, Carrier SJ, Strnad R et al (2019) Children can foster climate change concern among their parents. Nat Clim Chang 9:458–462. https://doi.org/10.1038/s41558-019-0463-3
Mertes H, Schoierer J, Gutknecht T, Hieronimi A, Mambrey V, Schmidt I, Böse-O’Reilly S, Lob-Corzilius T (2021) Climate change and health. Internist Prax 64:533–544
Milne S, Sheeran P, Orbell S (2000) Prediction and intervention in health-related behavior: a meta-analytic review of protection motivation theory. J Appl Soc Psychol 30:106–143. https://doi.org/10.1111/j.1559-1816.2000.tb02308.x
Mücke HG, Straff W, Faber M, Haftenberger M, Laußmann D, Scheidt-Nave C, Stark K (2013) Climate change and health: general framework on recommendations for action for public authorities and other stakeholders in Germany. https://edoc.rki.de/bitstream/handle/176904/295/298POD8uSatv6.pdf?sequence=1&isAllowed=y. Accessed 12 Dec 2022
Norman G (2010) Likert scales, levels of measurement and the “laws” of statistics. Adv Health Sci Educ 15:625–632. https://doi.org/10.1007/s10459-010-9222-y
Rai M, Stafoggia M, de’Donato F, Scortichini M, Zafeiratou S et al (2023) Heat-related cardiorespiratory mortality: effect modification by air pollution across 482 cities from 24 countries. Environ Int 174. https://doi.org/10.1016/j.envint.2023.107825
Schwarzer R (2016) Health Action Process Approach (HAPA) as a theoretical framework to understand behavior change. Actual en Psicol 30:119. https://doi.org/10.15517/ap.v30i121.23458
Semenza JC, Suk JE (2018) Vector-borne diseases and climate change: a European perspective. FEMS Microbiol Lett 365. https://doi.org/10.1093/femsle/fnx244
Stanley SK, Hogg TL, Leviston Z, Walker I (2021) From anger to action: differential impacts of eco-anxiety, eco-depression, and eco-anger on climate action and wellbeing. J Clim Chang Health 1:100003. https://doi.org/10.1016/j.joclim.2021.100003
Sullivan GM, Artino AR (2013) Analyzing and interpreting data from Likert-type scales. J Grad Med Educ 5:541–542. https://doi.org/10.4300/jgme-5-4-18
Team RC (2021) R: a language and environment for statistical computing. R Found. Stat. Comput. Vienna
Thielebein R, Stoltenberg U, Hirche W, Kestler J, Doil K et al (2019) Successful start - handout on education for sustainable development in child day care facilities. https://www.schleswig-holstein.de/DE/landesregierung/ministerien-behoerden/VIII/Service/Broschueren/Broschueren_VIII/Kita/Handreichung_Nachhaltige_Entwicklung.pdf?__blob=publicationFile&v=2. Accessed 22 Dec 2022
Traidl-Hoffmann C (2021) Allergologie. In: Traidl-Hoffmann C, Schulz C, Herrmann M, Simon B (eds) Planetary Health - Climate, environment, and health in the Anthopocene. Medizinisch Wissenschaftliche Verlagsgesellschaft, Berlin, pp 52–59
Ullrich S, Otto A, Thieken AH (2020) Dealing with heat in health and care facilities: survey of professional staff - selected results. https://www.uni-potsdam.de/fileadmin/projects/extrass/Hitzebefragung_Fachpersonal_online_final.pdf. Accessed 28 Dec 2022
Usher K, Durkin J, Bhullar N (2019) Eco-anxiety: how thinking about climate change-related environmental decline is affecting our mental health. Int J Ment Health Nurs 28:1233–1234. https://doi.org/10.1111/inm.12673
Watts N, Amann M, Arnell N, Ayeb-Karlsson S, Belesova K et al (2019) The 2019 report of The Lancet Countdown on health and climate change: ensuring that the health of a child born today is not defined by a changing climate. Lancet 394:1836–1878. https://doi.org/10.1016/S0140-6736(19)32596-6
Wolf M, Ölmez C, Schönthaler K, Porst L, Voß M, Linsenmeier M, Kahlenborn W, Dorsch L, Dudda L (2021) Climate impact and risk analysis 2021 for Germany. https://www.umweltbundesamt.de/sites/default/files/medien/479/publikationen/kwra2021_teilbericht_5_cluster_wirtschaft_gesundheit_bf_211027_0.pdf. Accessed 13 Dec 2022
Acknowledgements
The authors would like to thank the City of Munich for its cooperation in the study. We also thank the pedagogical staff who responded to our survey and shared their valuable knowledge with us.
Funding
Open Access funding enabled and organized by Projekt DEAL. Open access funding provided by Ludwig-Maximilians University Munich.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics approval
The study was approved by the Ethics Committee of the Medical Faculty of the Ludwig-Maximilians University Munich (project number 21-0843).
Conflict of interest
The authors declare no competing interests.
Additional information
Communicated by Angus Naylor
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Lehmann, H., Bose-O’Reilly, S., Schoierer, J. et al. Climate change-related health hazards in daycare centers in Munich, Germany: risk perception and adaptation measures. Reg Environ Change 23, 147 (2023). https://doi.org/10.1007/s10113-023-02136-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s10113-023-02136-w